The landscape of medical therapies is shifting faster than ever, and monoclonal antibodies (mAbs) are still holding their place center stage as some of the most promising and revolutionary therapeutic agents. Their exquisite specificity and tailored actions have not only made them a formidable weapon against diseases but have also catapulted them to the forefront of precision medicine.
The roots of mAbs reach back to the mid-1970s when César Milstein and Georges Köhler discovered a technique to produce antibodies in the lab. This groundbreaking research, which later earned them a Nobel Prize in Physiology or Medicine in 1984, paved the way for numerous applications in diagnostic tests, as well as therapeutic interventions.
In the decades that followed, monoclonal antibodies rapidly gained traction in the treatment of various ailments. The extreme specificity of antibodies in a natural environment is what has made them very interesting, initially for exact targeting of molecules involved in cancer.
Their applications expanded exponentially from autoimmune disorders such as rheumatoid arthritis and multiple sclerosis, to infectious diseases like Ebola and more recently, COVID-19. In fact, one of the moments in recent history that particularly showcased the versatility of monoclonal antibodies was their role in managing the COVID-19 pandemic. When traditional vaccines were still in development, mAbs were among the first therapeutic interventions available. They were able to neutralize the virus and played a critical role in the treatment of patients with severe COVID-19 symptoms.
More of a good thing
The first licenced monoclonal antibody was Orthoclone OKT3 (muromonab-CD3), approved in 1986 for use in preventing kidney transplant rejection. In the decades since more than 100 mAbs have been approved by the US Food and Drug Administration (FDA) for the treatment of different human diseases; apart from cancer they are also applied in autoimmune and chronic inflammatory diseases. Now the global monoclonal antibodies (MAbs) market is expected to grow from $168.70 billion in 2021 to $292.22 billion in 2026.
Over the decades that antibody manufacturing has been developing the process has achieved a degree of stability and manufacturing methods have matured, for example with cloned, standardized antibody-producing cells and a standard method for purification of the therapeutic antibody. Methods are so well-developed that variability has primarily been due to biological variations, but this has begun to change rapidly.
Even though the industry has had time to established reliable, consistent production processes, it seems that competition has rekindled an innovative spirit and drive.
This pioneering and successful application of monoclonal antibodies has inspired the development of many variants of the original antibodies, such as antibody fragments, bispecific antibodies, and derivatives such as antibody–drug conjugates, antibody–oligonucleotide conjugates, bispecific/multispecific antibodies, immunocytokines, antibody fragments, and scaffold proteins.
With mAbs becoming more numerous, diverse and complex, the downstream purification processes for isolating and purifying biological drugs is facing some real challenges in keeping up. (LINK TO NEW BIOPHARMACEUTICALS ON THE HORIZON ARTICLE)
One particularly tricky example is bispecific antibodies, where the challenge is to separate the drug which has two targets from its variants that have a single target. This usually results in lower yields and reduced purity and is not easy to solve.
Competition is driving the market
Current challenges facing the industry are primarily focused on accelerating time to market together with increasing flexibility and agility in manufacture to cope with increased numbers of products that usually require lower volumes that before. This is one of the major legacies of personalized medicine; many more drug variants are required, each with only a share of the patient population, but each demanding exactly the same stringency of development and manufacturing that has always applied. It is a great challenge indeed to adapt current pharmaceutical production strategies to these new demands.
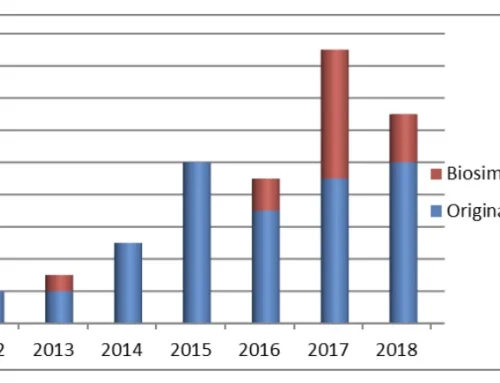
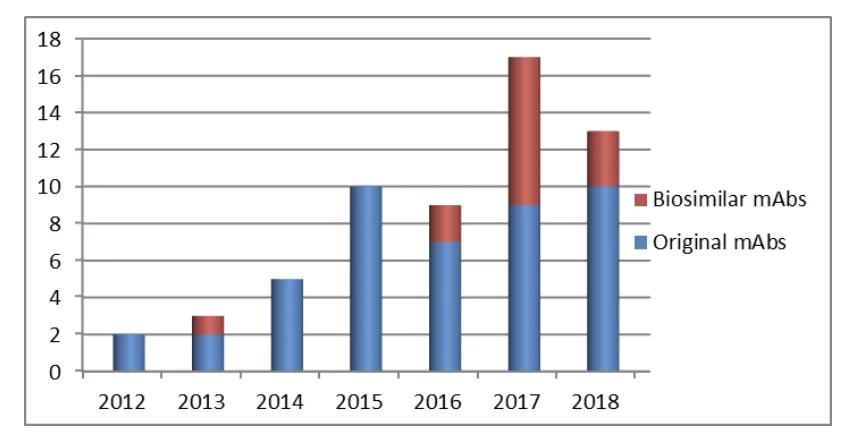
One specific, important challenge and driver of mAb market growth is cost reduction to address increased competition from biosimilars. Biosimilars are pharmaceuticals that are developed to have similar properties to a biological drug that has already been approved. A biosimilar mAb costs 20%-25% less than the originator drug.
Biosimilars hold the tantalizing promise of curbing increasing healthcare costs and satisfying economic pressure from patients and governments to reduce the cost of medication and increase access to treatment. For example, the requirement for clinical trials for a biosimilar is significantly lower than that of the original drug, a large contributor to the lower cost for a biosimilar.
In the coming years, we can also expect significant advances in diagnostics and understanding of disease mechanisms, resulting in more targeted treatment of cancers and other conditions. In conjunction with an increase in biosimilars, this would give a larger number of approved mAb products on a market which has, at the same time, a lower average annual demand.
So there is no reason for any slowing of the push towards more flexible, multi-product facilities and an ever-increasing diversity of mAb therapeutics to include greater numbers of ADCs, bispecifics, and FAb fragments.
The main variants of mAbs are becoming well-established therapeutics
The engineering of mAbs has become more sophisticated, allowing for the creation of molecules with improved therapeutic properties. For example, mAbs can be engineered to have longer half-lives, which means they remain in the body for longer periods of time and require less frequent dosing.
Antibody–drug conjugates (ADCs) combine the high specificity of antibodies with the potency of cytotoxic small molecules to deliver highly potent payloads within the targeted cell. An ADC comprises three main components: a mAb, cytotoxic payload, and linker.
The cytotoxic payload of an ADC is highly potent (from 100- to 1000-fold more toxic) compared to conventional chemotherapy which cannot be effectively administered due to extreme toxicity also for healthy tissue.
When it binds to a target antigen on tumor cells, an ADC can deliver the cytotoxin directly into the target cell cytoplasm, release the cytotoxic drug from the ADC during lysosomal degradation to destroy DNA or otherwise inhibit cell division and eventually kill tumor cells. These ”weaponized antibodies” can significantly improve the efficiency of cytotoxic molecules and reduce their off-target toxicity, a major issue of conventional cytotoxic chemotherapies. In recent years, the proposed use of ADCs has gradually gained steam, and they are rising stars in the tumor treatment field. (with 13 agents currently approved for the treatment of cancer).
Antibody–small interfering RNA (siRNA) conjugates (ARCs)
As of January 2023, four siRNA-based drugs have been approved by the FDA: patisiran, givosiran, lumasiran, and inclisiran. Since antibodies show high specificity and affinity toward overexpressed antigens in certain cell types or tissues, they are drawing increasing attention as suitable vehicles for siRNA delivery. It has actually been sixteen years since antibodies were first used to mediate the in vivo delivery of siRNAs via cell-surface receptors. siRNAs can be coupled with antibodies for treating cancer (breast cancer, prostate cancer, colon cancer and MM) or other diseases (HIV and leukemia).
But there are several issues in using ARCs that remain unsolved.
- ARCs do not readily enter cells because the negative charge of the appended siRNA.
- similar to other delivery systems, endosomal escape is a major obstacle for intracellular delivery of siRNAs, leading to inefficient localization of siRNAs into the cytoplasmic RISC.
- the targeted antigen determines the efficiency of siRNA delivery. For example, Fab-type ARCs have only been proven effective against TfR1,91 a receptor prevalent in the endocytic pathway.
- lack of quantitative approaches for investigating endosomal escape of siRNAs (released from ARCs) and interaction of siRNAs with the RISC machinery.
- steric hindrance created during the conjugation of antibodies with a siRNA lowers conjugation efficiency.
- with current technology, the ADC linker cannot simply be simply grafted into the conjugate. Extensive linker optimization is needed to generate certain ARCs.
With the boom in ADC production, the strategic use of ARCs, which is similar to the rationale of ADC use, is expected to create new opportunities for the targeted interference of gene expression in multiple organs in vivo in the near future.
Multispecific antibodies to address a multi-cause, complex disease
Miniaturization and multifunctionalization represent two major directions in antibody development. Full-length antibodies have been transformed into fragments, e.g., Fabs, scFvs, and VHH domains, and small scaffold proteins (e.g. affibodies and DARPins).
And fragments have been combined to create multifunctional therapeutics, primarily driven by the sheer complexity of causes of cancer which will always limit the efficacy of any monospecific-based cancer treatment.
The original concept of mixing univalent antibody fragments to generate multispecific antibodies was first described in the 1960s by Nisonoff and colleagues. Initially, bispecific Abs were generated by chemical conjugation of two antibody fragments and then by somatic cell fusion of two different hybridoma cell lines. The development of recombinant DNA technology and antibody engineering technology made it possible to assemble different antibody domains into various formats of multispecific antibodies with a desired orientation and stability. There are two major categories of multispecific antibody formats: IgG-like antibodies (with an Fc domain) and non-IgG-like antibodies (without an Fc domain).
For over three decades, multispecific antibodies have received tremendous attention to address unmet clinical needs. A broad variety of multispecific antibody formats has been developed to function through different mechanisms in cancer immunotherapy, including engaging T cells or other immune cells to specifically kill tumor cells, bridging receptors to block or activate linked signaling pathways, and targeting multiple tumor antigens or different epitopes on tumor cells to increase tumor selectivity.
With advancements in biotechnology and our understanding of diseases at the molecular level, mAbs will likely become even more targeted and effective. In addition, their role in personalized medicine is ready to grow, as they enable therapies tailored to an individual’s unique genetic and molecular profile.
In parallel, novel drug delivery methods, such as nanoparticle-based systems, are expected to enhance the potential of monoclonal antibodies by improving their delivery and effectiveness. These advancements indicate that we are only beginning to scratch the surface of what these versatile molecules can achieve.
{kind=link}
{kind=link}
{kind=link}
Leave A Comment